
Last Aid Training Online: Participants’ and Facilitators’ Perceptions from a Mixed-Methods Study in Rural Scotland

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.1.1. LAT Participants
2.1.2. LAT Facilitators
2.2. Data Collection
2.2.1. Online Survey
2.2.2. Interviews
2.3. Data Analysis
3. Results
- Participant perceptions of their knowledge, confidence, and experiences providing end-of-life care
- Participant perspectives on the online delivery of LAT and facilitator experiences of delivering LAT in online and offline settings.
3.1. Participant Perceptions of Their Knowledge, Confidence, and Experiences Providing End-of-Life Care
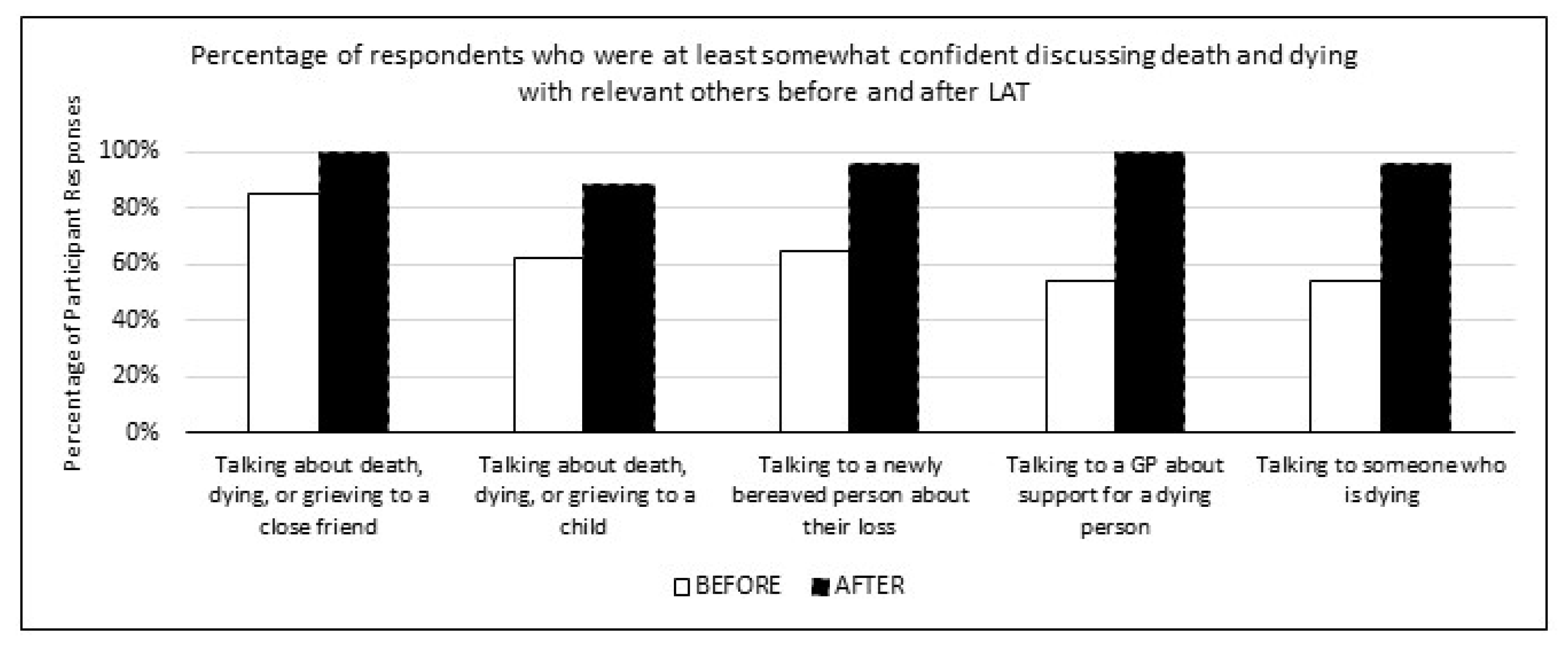
3.1.1. Knowledge and Experiences Talking about Death and Dying
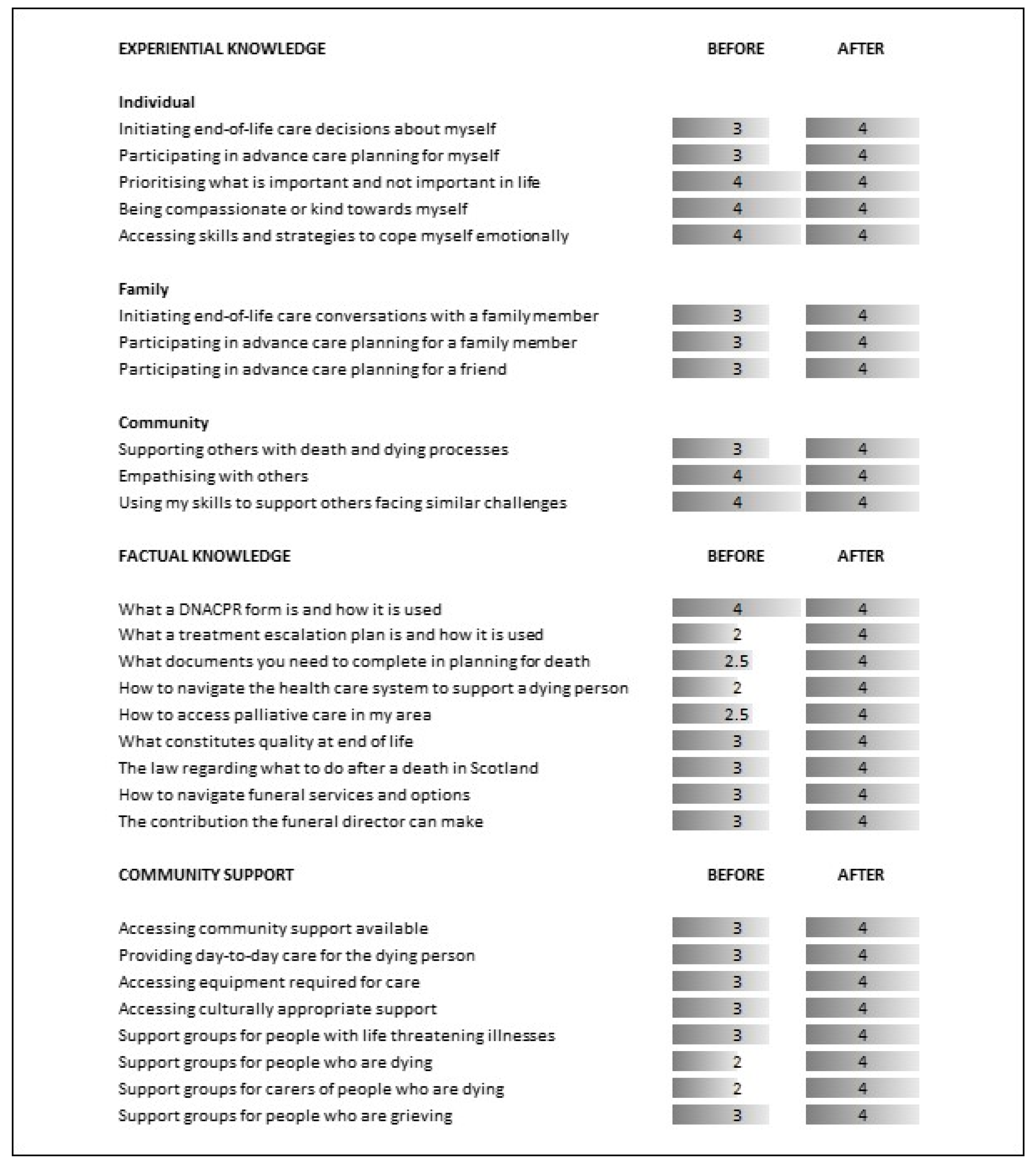
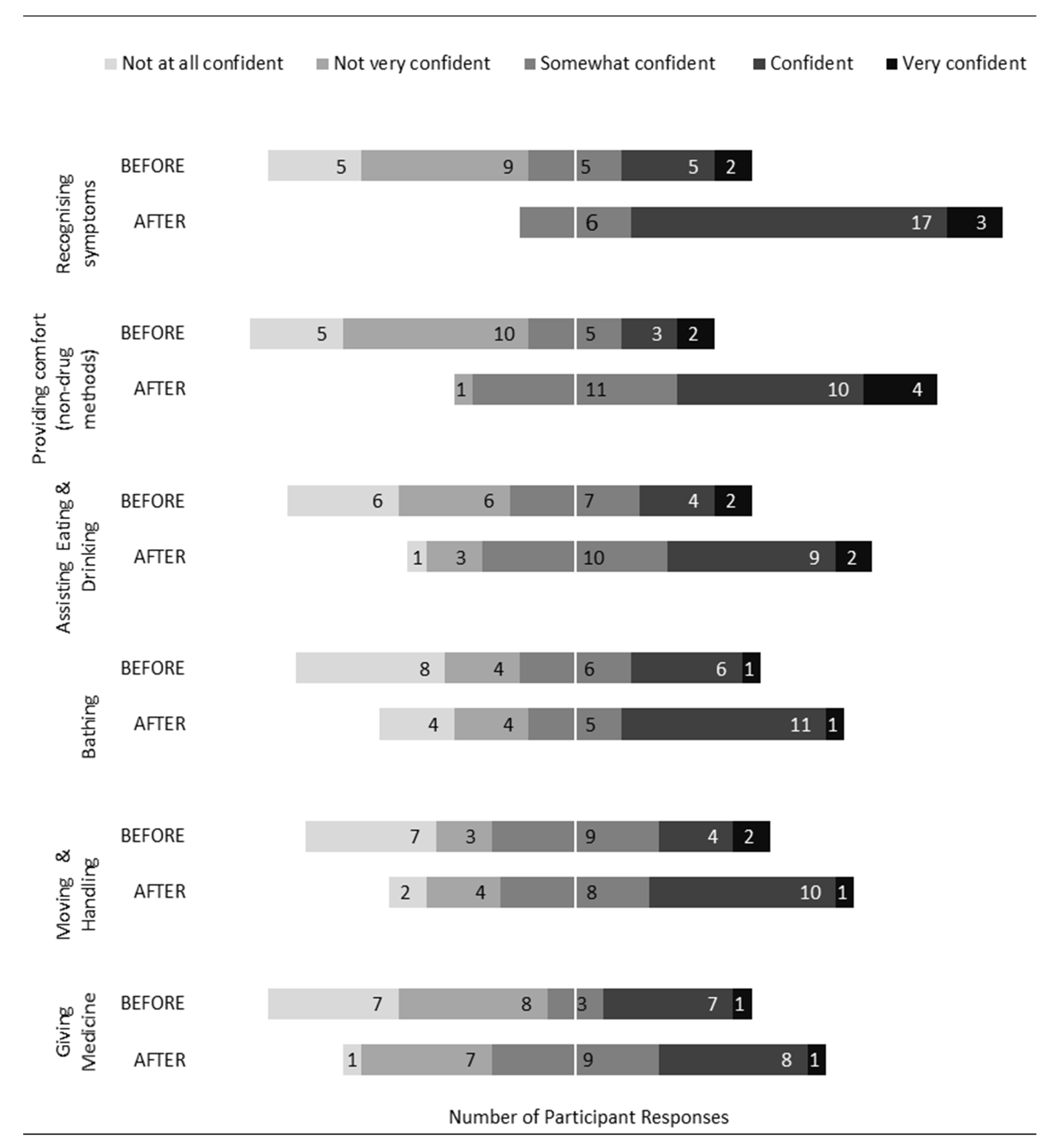
3.1.2. Knowledge and Confidence around Death and Dying
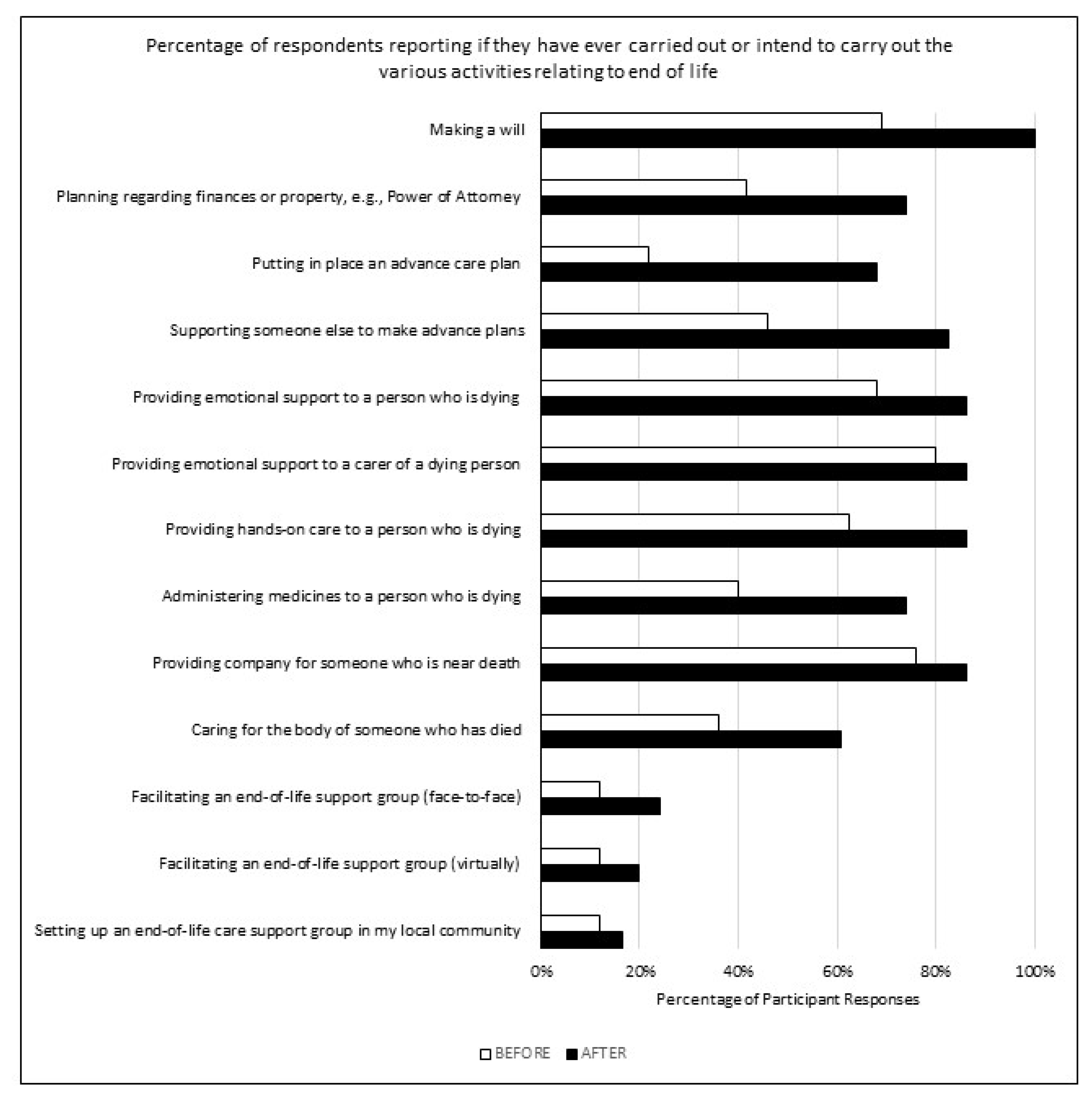
3.2. Decisions and Intentions to Support End-of-Life Care Needs
3.3. Overall Impact of LAT on Participants
3.3.1. Demystifying Palliative Care and Enhancing Understanding
“I don’t know about not understanding about it but from a personal, life … somebody who was ill in my own family and obviously I didn’t know what to expect then, but by the end of this training I learnt much more about it and it made me understand what I went through … and if this ever happened again, I’d have a greater understanding, it helped me deal with it”.(Interview Participant 3)
“Well, the main thing was that I learnt more (…) various stages, how you should not be frightened of it. And it’s…just a good (…) thing for you to learn, you know more about what may happen and also afterwards, like the grieving bit, there’s no right or wrong way that people grieve”.(Interview Participant 3)
3.3.2. Creating Normalised Conversations around Death and Dying
“How positive it is for society to have accepted that it’s a good, kind, loving thing to be able to talk about death”.[Survey respondent 4]
“I already know and already talk about these things but as I say, I think the course did make me think ‘yeah, we need to talk about them more frequently and not when it’s about to happen’, you know, you need to talk about them just over Sunday dinner when nobody is dying. That’s probably the key thing; let’s not wait until it’s needed, let’s talk about it all the time.”(Interview Participant 11)
“I would say because of the current situation again I have not really had much opportunity to. Not a matter or bias to the course, I mean, it’s only been a matter of weeks and we’ve not had the opportunity to put any of these choices into practice”(Interview Participant 10)
3.3.3. Thinking Ahead and Advocating for Self and Others
“I don’t have power of attorney and that’s the thing that we talked about quite a lot. So yes, it’s made me think very seriously about that and in fact my husband and I have been speaking about that. I teach it but I don’t do what I preach.”(Interview Participant 5)
“I am a great advocate of conversations and I know that they don’t happen, people don’t want to talk about death or dying, I am quite an advocate that people need to do that. So, it almost gave me permission to carry on doing that.”(Interview Participant 5)
“There were certain things that we talked about that were more vague ideas that are now relatively clear as far as knowing what would need to be done. And in terms of my own life, it’s put into focus that my wife and I should start looking at things like getting wills and things like that, regardless of the fact that we’re only in our mid-thirties, it’s never too early.”(Interview Participant 9)
3.4. Participants’ and Facilitators’ Perceptions and Experiences of LAT within the Virtual Online Environment
3.4.1. Accessibility
“We can’t physically manage to take presenters and take facilitators out to small rural communities in the Highlands. Highlands geographically—it’s so difficult. And there is a lot to learn, I suspect, from doing it on Zoom—doing it online—in terms of taking it out to people in little remote rural communities, where they don’t have access to anything. I do think that online sessions in all sorts of areas have a huge potential.”(Interview Participant 7)
It was a good mix of being interactive with trainers and other participants and engaging solo through listening or reading. The trainers were very approachable and relatable.[Survey respondent 5]
Ability to attend! I probably wouldn’t have found the time otherwise. Home comfort. Being able to take notes without feeling rude or not present.[Survey respondent 6]
“We’ve got to learn how to use them and to learn how to get the best out of them—and it’s a steep learning curve and an uphill struggle.”(Interview Participant 7)
3.4.2. Desired Diversification
Content could do more to recognise secular philosophical aspects of death/dying & life/living, as well as addressing issues surrounding death/dying and caring for someone who is dying in circumstances where partnership is non-traditional, i.e., LGBTQIA+ relationships.[Survey respondent 7]
“something I think could be improved, in the way they want to take it out to general communities and things, was it was very, very heavily about—the context of the death that they were talking about was very much a predicted, expected planned death and I guess there’s room for that course to be much wider, to include people having at least some thoughts and discussions about what if somebody doesn’t die in a predicted or expected way.”(Interview Participant 11)
“I think a script. Although now, it’s funny … the more I think about that now, actually I wouldn’t like that because I’ve tried using other people’s notes and I just re-write them because they are not my words, they are not how I would say it. So there was a handbook and it was being translated but actually I would still want my own notes because that’s not how I would say it, it’s not me, so it doesn’t sit comfortably for me to say it that way.”(Interview Participant 6)
3.4.3. Connectedness
“If I were speaking to somebody who was about to take the training and didn’t know what to expect I’d say, ‘don’t worry, you are not going to leave curled up in a ball in fear of the unknown’, it’s … you know, obviously it’s a topic that’s difficult for a lot of people to discuss but I feel that it was done in such a way it was as sensitive to that as it could have been and it was, the information that was provided it helped to disarm the topic a bit. It made the subject a little bit less scary, I guess.”(Interview Participant 9)
“Just so people are willing to share this very private part of their lives and to open up the conversation about dying … it’s part of a bigger, national movement to talk about death and dying as a normal part of life. And sometimes I’d like to be just a little fly on the wall in the corner of the room just looking down on that conversation because you just don’t appreciate sometimes how profound that is, I think we take it for granted that these people are opening up their lives in the little TV screen in their living room for that short time. And then they are gone, they click a button, and they are gone, and you have no more connection with that person ever again, but you just had that little opportunity to just drop something positive into their experience and hopefully help them along the way.”(Interview Participant 1)
“Subject is difficult and emotional—delivering the course online removes the element of human contact and support that some may find helpful in dealing with these matters, even in an educational setting”.[Survey respondent 7]
“… you can have these really honest conversations when you are face-to-face and you can say to them, if you need a minute you can go out and you can read people’s emotions”.(Interview Participant 2)
“In a room, you can go round afterwards and say, ‘Do you want to look at the pieces of paper?’ and chat to people. Or pick out someone who’s been uncomfortable, or the quiet one in the corner who’s said very little. You’ve got that ability to relate to people that you just don’t have on screen.”(Interview Participant 7)
“an improvement to the course, I think, would be to actually get people to have that conversation perhaps in pairs, we did go into little break-out rooms, as can often be the case, people talked about other things and kind of avoided talking about the thing that wanted to be talked about … make it longer and enable people to really have more interaction and more discussion between each other and between themselves and kind of test out having some of these conversations”(Interview Participant 11)
“it would have been quite nice to have been with other people that were not clinical. That’s the only…I know you just can’t control that and, as I say, I know a few people couldn’t link in that day so there may have been people within that but personally, for me, that would have been good to hear from their viewpoint as well”(Interview Participant 5)
“And again it kind of begs that question to me, that I’ve obviously got a bit stuck on, is that because they are copyrighted in some way, I mean why on earth would you not give people the slides if they are on a course? It just seems completely wrong to me.”(Interview Participant 11)
3.4.4. Discomfort and Difficulties
“I feel that it’s given me a bit more confidence and knowledge behind it and it’s certainly facilitated conversations in my own life”.(Interview Participant 2)
“I think my expectations were that we would probably get a script that we were going to use when we were actually facilitating the sessions. Especially when I don’t have a clinical background and I don’t have a knowledge of end-of-life care in the same way: I see it as a bystander. So I did think we would get a training manual … Definitely a script that would help”.(Interview Participant 6)
“I feel self-conscious with the technology, I feel it takes away a little bit of my personality, my ability to be my real self because I’m self-conscious. So I think probably in-person but I do see the need for the technology”.(Interview Participant 1)
“I just need to keep delivering the material regularly so I can keep up my skills. One of my worries is if they take on board too many new facilitators then we all end up just doing one course a year or something. That will just be pointless to me, I think to keep your skills up and your … you tuned in to it, I think you have to keep doing it regularly”.(Interview Participant 1)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finucane, A.M.; Bone, A.E.; Etkind, S.; Carr, D.; Meade, R.; Munoz-Arroyo, R.; Moine, S.; Iyayi-Igbinovia, A.; Evans, C.J.; Higginson, I.J.; et al. How many people will need palliative care in Scotland by 2040? A mixed-method study of projected palliative care need and recommendations for service delivery. BMJ Open 2021, 11, e041317. [Google Scholar] [CrossRef] [PubMed]
- Finucane, A.M.; Bone, A.E.; Evans, C.J.; Gomes, B.; Meade, R.; Higginson, I.J.; Murray, S.A. The impact of population ageing on end-of-life care in Scotland: Projections of place of death and recommendations for future service provision. BMC Palliat. Care 2019, 18, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellehear, A.; O’Connor, D. Health-promoting palliative care: A practice example. Crit. Public Health 2008, 18, 111–115. [Google Scholar] [CrossRef]
- World Health Organization. Ottawa Charter for Health Promotion; WHO/EURO: 1986-4044-43803-61677; WHO: Copenhagen, Denmark, 1986. [Google Scholar]
- Wegleitner, K.; Heimerl, K.; Kellehear, A. Compassionate Communities; Routledge key themes in health and society; Routledge: London, UK, 2015. [Google Scholar]
- Strategic Framework for Action on Palliative and End of Life Care 2016–2021; Scottish Government Health and Community Care: Edinburgh, UK, 2015.
- Noonan, K.; Horsfall, D.; Leonard, R.; Rosenberg, J. Developing death literacy. Prog. Palliat. Care 2016, 24, 31–35. [Google Scholar] [CrossRef]
- Mills, J.; Rosenberg, J.P.; Bollig, G.; Haberecht, J. Last Aid and Public Health Palliative Care: Towards the development of personal skills and strengthened community action. Prog. Palliat. Care 2020, 28, 343–345. [Google Scholar] [CrossRef]
- Sallnow, L.; Smith, R.; Ahmedzai, S.H.; Bhadelia, A.; Chamberlain, C.; Cong, Y.; Doble, B.; Dullie, L.; Durie, R.; Finkelstein, E.A.; et al. Report of the Lancet Commission on the Value of Death: Bringing death back into life. Lancet 2022, 399, 837–884. [Google Scholar] [CrossRef]
- Bollig, G.; Heller, A. The last aid course-a simple and effective concept to teach the public about palliative care and to enhance the public discussion about death and dying. Austin Palliat. Care 2016, 1, 1010. [Google Scholar]
- Bollig, G.; Brandt, F.; Ciurlionis, M.; Knopf, B. Last Aid Course. An education for all citizens and an ingredient of compassionate communities. Healthcare 2019, 7, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, S.; Sallnow, L. Public health approaches to end-of-life care in the UK: An online survey of palliative care services. BMJ Support. Palliat. Care 2013, 3, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Bollig, G.; Brandt Kristensen, F.; Wolff, D.L. Citizens appreciate talking about death and learning end-of-life care–A mixed-methods study on views and experiences of 5469 Last Aid Course participants. Prog. Palliat. Care 2021, 29, 140–148. [Google Scholar] [CrossRef]
- Bollig, G.; Meyer, S.; Knopf, B.; Schmidt, M.; Hayes Bauer, E. First Experiences with Online Last Aid Courses for Public Palliative Care Education during the COVID-19 Pandemic. Healthcare 2021, 9, 172. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R.; Noonan, K.; Horsfall, D.; Psychogios, H.; Kelly, M.; Rosenberg, J.P.; Rumbold, B.; Grindrod, A.; Read, N.; Rahn, A. Death Literacy Index: A Report on Its Development and Implementation; Western Sydney University: Penrith, UK, 2020. [Google Scholar]
- JISC. JISC Online Surveys. 2021. Available online: https://www.jisc.ac.uk/online-surveys/ (accessed on 22 April 2021).
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Abel, J.; Kellehear, A.; Millington Sanders, C.; Taubert, M.; Kingston, H. Advance care planning re-imagined: A needed shift for COVID times and beyond. Palliat. Care Soc. Pract. 2020, 14, 2632352420934491. [Google Scholar] [CrossRef] [PubMed]
- Oliver, D. David Oliver: Detoxifying DNACPR decisions. BMJ 2020, 371, m4069. [Google Scholar] [CrossRef] [PubMed]
- Andershed, B.; Ternestedt, B. Development of a theoretical framework describing relatives’ involvement in palliative care. J. Adv. Nurs. 2001, 34, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Sallnow, L.; Richardson, H.; Murray, S.A.; Kellehear, A. The impact of a new public health approach to end-of-life care: A systematic review. Palliat. Med. 2016, 30, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Sallnow, L.; Paul, S. Understanding community engagement in end-of-life care: Developing conceptual clarity. Crit. Public Health 2015, 25, 231–238. [Google Scholar] [CrossRef]
- Kars, M.C.; van Thiel, G.J.; van der Graaf, R.; Moors, M.; de Graeff, A.; van Delden, J.J. A systematic review of reasons for gatekeeping in palliative care research. Palliat. Med. 2016, 30, 533–548. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | N | % | Gender | N | % |
| 18–24 years | 1 | 3.8 | Male | 3 | 11.5 |
| 25–34 years | 2 | 7.7 | Female | 22 | 84.6 |
| 35–44 years | 4 | 15.4 | Rather not say | 1 | 3.8 |
| 45–54 years | 9 | 34.6 | |||
| 55–64 years | 6 | 23.1 | |||
| 65–79 years | 4 | 15.4 | |||
| Education | N | % | Employment | N | % |
| National 5 or equivalent | 1 | 3.8 | Employed—full-time | 10 | 38.5 |
| Highers or equivalent | 2 | 7.7 | Employed—part-time | 9 | 34.6 |
| Certificate or Diploma | 5 | 19.2 | Self-employed | 2 | 7.7 |
| Undergraduate degree | 8 | 30.8 | Retired | 4 | 15.4 |
| Postgraduate degree | 7 | 26.9 | Student | 1 | 3.8 |
| Rather not say | 3 | 11.5 | |||
| Employer | N | % | Residence | N | % |
| NHS | 6 | 23.1 | Urban area | 10 | 38.5 |
| Social Care | 1 | 3.8 | Semi-Urban area | 4 | 15.4 |
| Third Sector | 4 | 15.4 | Rural area | 5 | 19.2 |
| Education | 7 | 26.9 | Remote area | 2 | 7.7 |
| Other | 8 | 30.8 | Semi-Rural area | 5 | 19.2 |
| Relationship Status | N | % | Networks | N | % |
| Married | 15 | 57.7 | Family | 22 | 84.6 |
| Never married | 2 | 7.7 | Neighbours | 9 | 34.6 |
| Widowed | 2 | 7.7 | Community Groups | 7 | 26.9 |
| Divorced | 1 | 3.8 | Religious Groups | 5 | 19.2 |
| Separated (not divorced) | 1 | 3.8 | Friends | 22 | 84.6 |
| Partnered (not living together) | 1 | 3.8 | |||
| Single | 2 | 7.7 | |||
| Other | 2 | 7.7 | |||
| Reason for Attendance | N | % | Source of Access | N | % |
| Personal interest | 21 | 80.8 | Family | 1 | 3.8 |
| COVID-19 | 1 | 3.8 | Colleague | 10 | 38.5 |
| Long-term condition | 1 | 3.8 | 3 | 11.5 | |
| Terminal illness | 1 | 3.8 | Social Media | 4 | 15.4 |
| Related to work | 16 | 61.5 | Hospice Newsletter/Website | 11 | 42.3 |
| Background and Experience | N | % | |
|---|---|---|---|
| Religious/Spiritual Background | Yes | 13 | 50.0 |
| No | 12 | 46.2 | |
| Rather not say | 1 | 3.8 | |
| Religious/Spiritual Practice | Yes | 10 | 38.5 |
| No | 15 | 57.7 | |
| Rather not say | 1 | 3.8 | |
| Experience with people at end of life—Paid | Yes | 10 | 38.5 |
| No | 16 | 61.5 | |
| Experience with people at end of life—Volunteer | Yes | 10 | 38.5 |
| No | 16 | 61.5 | |
| Work experience with grief and loss | Yes | 13 | 50.0 |
| No | 13 | 50.0 | |
| Volunteer experience with grief and loss | Yes | 12 | 46.2 |
| No | 14 | 53.8 | |
| Previous training on dying, grief, or bereavement | Yes | 15 | 57.7 |
| No | 11 | 42.3 |
| Talking about Death & Dying | Time Point | Agree (%) | Disagree (%) | Unsure (%) | NA (%) |
|---|---|---|---|---|---|
| We discuss death and dying in my family | 1 | 57.8 | 38.4 | 0.0 | 3.8 |
| 2 | 77.0 | 15.4 | 3.8 | 3.8 | |
| We discuss death and dying in my community | 1 | 30.8 | 53.8 | 15.4 | 0.0 |
| 2 | 50.0 | 38.5 | 11.5 | 0.0 | |
| We discuss death and dying in my workplace | 1 | 46.2 | 34.6 | 3.8 | 15.4 |
| 2 | 57.7 | 26.9 | 3.8 | 11.5 | |
| We discuss death and dying in my church/ religious gathering | 1 | 34.6 | 0.0 | 0.0 | 65.4 |
| 2 | 34.6 | 0.0 | 0.0 | 65.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macaden, L.; Broadfoot, K.; Carolan, C.; Muirhead, K.; Neylon, S.; Keen, J. Last Aid Training Online: Participants’ and Facilitators’ Perceptions from a Mixed-Methods Study in Rural Scotland. Healthcare 2022, 10, 918. https://doi.org/10.3390/healthcare10050918
Macaden L, Broadfoot K, Carolan C, Muirhead K, Neylon S, Keen J. Last Aid Training Online: Participants’ and Facilitators’ Perceptions from a Mixed-Methods Study in Rural Scotland. Healthcare. 2022; 10(5):918. https://doi.org/10.3390/healthcare10050918
Chicago/Turabian StyleMacaden, Leah, Kirsten Broadfoot, Clare Carolan, Kevin Muirhead, Siobhan Neylon, and Jeremy Keen. 2022. "Last Aid Training Online: Participants’ and Facilitators’ Perceptions from a Mixed-Methods Study in Rural Scotland" Healthcare 10, no. 5: 918. https://doi.org/10.3390/healthcare10050918